Location
Date
Author
eli fessler
Licensed under a Creative Commons Attribution 4.0 License.
Tags
No tags
Text
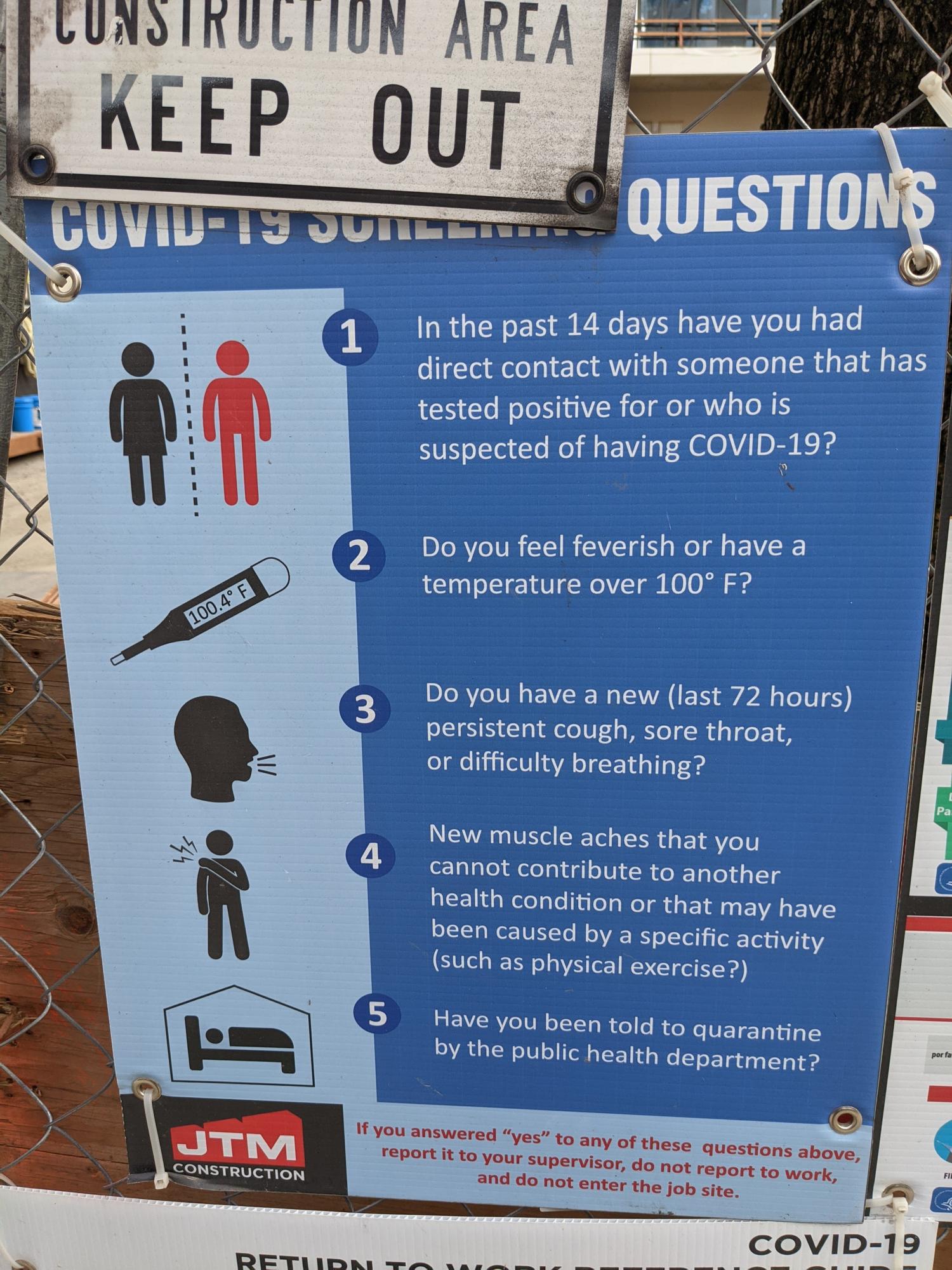
COVID-19 SCREENING QUESTIONS 1 In the past 14 days have you had direct contact with someone that has tested positive for or who is suspected of having COVID-19? 2 Do you feel feverish or have a temperature over 100° F? 3 Do you have a new (last 72 hours) persistent cough, sore throat, or difficulty breathing? 4 New muscle aches that you cannot contribute to another health condition or that may have been caused by a specific activity (such as physical exercise?) 5 Have you been told to <...>